Here just we want to discuss about diagnostic aspects ...
#1- This ECG shows Diffuse ST-Segment Depression ( V2-v6 with upright T waves ) . Left Axis deviation . Normal Sinus Rhythm . Tall R wave in V1=RBBB with is new too .R>S in V1-v4 and ST-Depression with upright Ts. No considerable ST changes in II, III and VF. Troponin Elevated 4+. Echo= Inferior-Mid anterior.septal RWMA.

#2- These changes are favoring Acute True Posterior Wall ST-elevation MI . but in True Posterior the changes just only confined to the v1-v3, and we have RBBB which is fresh onset and inferior leads ( II, III and VF) are about normal then what should be suspected?
#3- Now we are suspecting RCA±LCx mostly but there are also some feature of Left Main and LAD in our suspicion ? Now how to reach the Dx.?
#4- The accurate characteristics of Left Main involvements are : Lead aVR ST elevation and infero-lateral ST depression, the presence of ST depression >0.1mV in eight or more leads , couple with ST elevation in aVR and/or V1 .HERE WE HAVE NOT ANY AS SUCH CRITERIA TO MATCH WITH THIS ,THEREFORE, THE LEFT MAIN RULES OUT.
#5- We have here the exact criteria for true Posterior wall MI , but initial Q waves and recent onset RBBB makes the case tough . so we can say there is True posterior ! but something especial is also there , and what is this ?
#6- Pericardial Q waves favoring Ant-septal MI ! So once we can say there are anterior and Posterior MI . Recent onset RBBB favors anterior wall MI on other hand Tall R in V1 shows Q wave in posterior which we have both anterior and posterior changes at the same time and echo adding to this suspicion . so but why inferior leads are spared , in Posterior wall MI there must be Inferior leads changes. next step is angiography ?

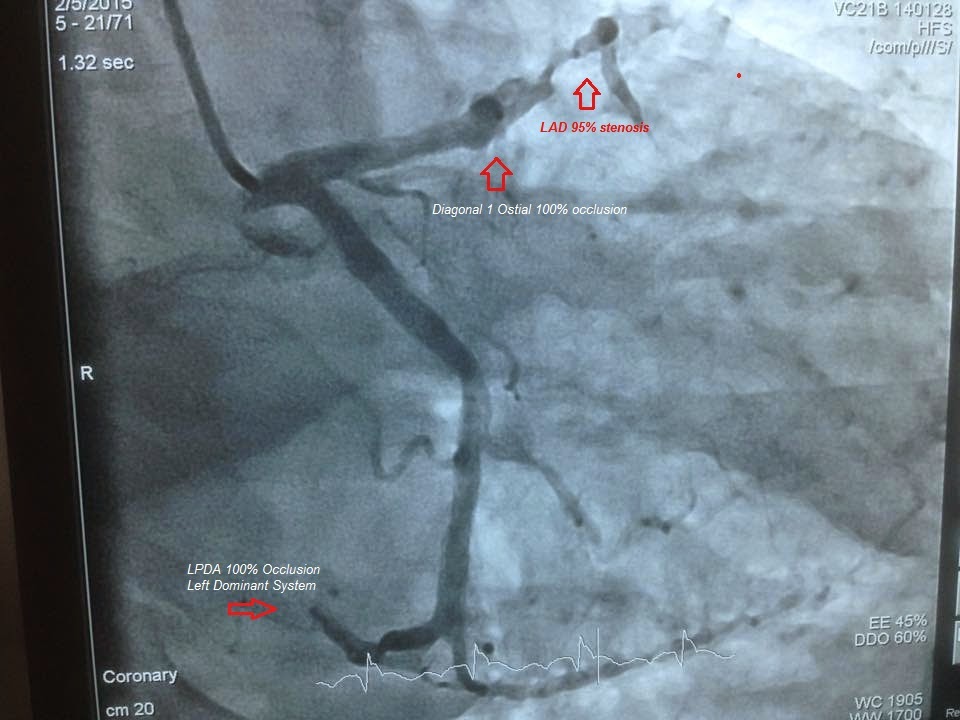


#7- Angiography shows Small Non-dominant RCA ! and it is 100% CTO, so when there is non-dominant it has no value ! and we see Left posterior descending artery arising from LCx showing left dominant then LPDA is also 100% acutely occluded , and LAD Mid is 95% occluded and D1 is 100% ostial occlusion !
#8- Result- Echo+ECG shown Anterior and Posterior wall MI . Angiography did show that this patient have acute Posterior and Anterior wall simultaneously but this True posterior is the result of LPDA not RCA , and anterior is due to LAD and D1.
#1- This ECG shows Diffuse ST-Segment Depression ( V2-v6 with upright T waves ) . Left Axis deviation . Normal Sinus Rhythm . Tall R wave in V1=RBBB with is new too .R>S in V1-v4 and ST-Depression with upright Ts. No considerable ST changes in II, III and VF. Troponin Elevated 4+. Echo= Inferior-Mid anterior.septal RWMA.
#2- These changes are favoring Acute True Posterior Wall ST-elevation MI . but in True Posterior the changes just only confined to the v1-v3, and we have RBBB which is fresh onset and inferior leads ( II, III and VF) are about normal then what should be suspected?
#3- Now we are suspecting RCA±LCx mostly but there are also some feature of Left Main and LAD in our suspicion ? Now how to reach the Dx.?
#4- The accurate characteristics of Left Main involvements are : Lead aVR ST elevation and infero-lateral ST depression, the presence of ST depression >0.1mV in eight or more leads , couple with ST elevation in aVR and/or V1 .HERE WE HAVE NOT ANY AS SUCH CRITERIA TO MATCH WITH THIS ,THEREFORE, THE LEFT MAIN RULES OUT.
#5- We have here the exact criteria for true Posterior wall MI , but initial Q waves and recent onset RBBB makes the case tough . so we can say there is True posterior ! but something especial is also there , and what is this ?
#6- Pericardial Q waves favoring Ant-septal MI ! So once we can say there are anterior and Posterior MI . Recent onset RBBB favors anterior wall MI on other hand Tall R in V1 shows Q wave in posterior which we have both anterior and posterior changes at the same time and echo adding to this suspicion . so but why inferior leads are spared , in Posterior wall MI there must be Inferior leads changes. next step is angiography ?
#7- Angiography shows Small Non-dominant RCA ! and it is 100% CTO, so when there is non-dominant it has no value ! and we see Left posterior descending artery arising from LCx showing left dominant then LPDA is also 100% acutely occluded , and LAD Mid is 95% occluded and D1 is 100% ostial occlusion !
#8- Result- Echo+ECG shown Anterior and Posterior wall MI . Angiography did show that this patient have acute Posterior and Anterior wall simultaneously but this True posterior is the result of LPDA not RCA , and anterior is due to LAD and D1.





